
SPOTLIGHT
Experts call for better screening and treatment of TB during pregnancy

Falling ill with tuberculosis can be challenging for anyone, but it can be especially hard if you are pregnant or have just given birth. Globally, TB is among the top five causes of death in women of child-bearing age. Tiyese Jeranji spoke to experts about the risks, challenges and ongoing studies on maternal TB.
Busisiwe Beko, from Khayelitsha in Cape Town, was diagnosed with drug-resistant tuberculosis (DR-TB) while she was pregnant. She remembers it as a very difficult period in her life.
“The time that I was diagnosed with TB was the time that I found out I had HIV. In that period, it was really a struggle for me, because I also found out I was pregnant. It was so unfortunate that I couldn’t produce sputum so that I could be tested for TB. That was the first challenge for me,” says Beko, who now works for Doctors Without Borders (MSF). Beko shared her experience during a session on maternal TB at the recent Union World Conference on Lung Health.
Shortly after delivery, she was told her baby had also contracted DR-TB.
“It was also a challenge for my child. She had the same strain [as] I did. When she was admitted [to] the hospital, it was far from Khayelitsha. I wasn’t allowed in the ward because it was a paediatric ward, so it was difficult for me to see her. She also had to get injections every day. It was painful watching my child get the injection. When she used to cry, I also used to cry.”
Beko says that during this time she did not receive any counselling, which would have helped prepare her for what lay ahead.
“I was on medication and I had to take [an] injection every day. Sometimes I would feel very nauseous and sometimes I would vomit. The side-effects were really bad,” she says.
But the treatment worked and Beko survived, which cannot be said for everyone who falls ill with TB during or after a pregnancy.
TB is among the top five causes of death in women of child-bearing age around the world. In 2021, the World Health Organization (WHO) estimated that 3.4 million women globally fell ill with TB, though it is not known how many of them were pregnant at the time. Indeed, little is known about the true burden of maternal TB.
Difficult to diagnose
Hendrik Simon Schaaf, distinguished professor and senior specialist in the Department of Paediatrics and Child Health at Stellenbosch University, explains that maternal TB is when someone becomes ill with TB during pregnancy or during the postnatal period.
“It is quite difficult to diagnose TB during pregnancy,” he says. “Women may be asymptomatic or may experience symptoms as part of pregnancy, which may be similar to that of TB. The WHO has a symptomatic screening recommendation of fever, cough, night sweats and loss of weight for TB in pregnancy, but this symptom screening does not perform well during pregnancy.”

Dr Francesca Conradie. (Photo: Supplied / Spotlight)
Schaaf says clinicians are reluctant to do chest X-rays during pregnancy because of fear of radiation to the foetus, but this is likely to be unfounded if the mother’s womb is properly protected (shielded).
“TB is a progressive disease,” he says. “So, if the mother is not treated during pregnancy, the disease can progress and cause severe illness and even death – so for mothers themselves it is important to be treated.”
Idah Mokhele, an epidemiologist and senior researcher at the Health Economics and Epidemiology Research Office (HE2RO), stresses that the perinatal period is an important opportunity to screen, diagnose and treat those at high risk for TB. Mokhele says TB may be transmitted from mother to child in utero, intrapartum and postpartum.
Because TB in pregnancy is difficult to diagnose due to the similarity of TB symptoms and those of pregnancy, she says diagnosis and treatment delays are common, which exacerbates adverse maternal, pregnancy and infant outcomes. “That is why it’s important to integrate active TB case-finding in antenatal care to ensure early diagnosis and treatment of infected mothers.”
Adverse outcomes
According to Dr Marian Loveday, senior scientist at the South African Medical Research Council, in terms of the mother, “TB is a leading cause of non-obstetric maternal death, particularly in the context of HIV infection. In South Africa, it is the leading cause of non-obstetric death.”
In maternal TB, unfavourable TB outcomes (treatment failure, loss to follow-up, death) are more likely compared with women who are not pregnant, Loveday tells Spotlight.
“Maternal TB is also associated with increased rates of anaemia, pre-eclampsia, postpartum haemorrhage and hospitalisation. Pregnancies affected by TB have higher rates of miscarriage, stillbirth, prematurity, intra-uterine growth restriction and perinatal asphyxia. [And] adverse infant outcomes include prematurity and low birth weight (less than 2,500g) and prolonged hospitalisation,” says Loveday.
She says if the mother has been on appropriate treatment for at least two weeks and is taking her treatment, she is unlikely to be infectious, so the chance of transmitting TB to the newborn is unlikely.
However, undiagnosed maternal TB posed a significant risk to infants.
Visit Daily Maverick’s home page for more news, analysis and investigations
“Due to immune immaturity, there is a 30% to 80% risk of transmission to an infant from a mother or household contact with infectious TB and perinatal TB has a mortality greater than 11%. These risks are increased in the context of HIV exposure and infection. Infant prophylaxis (TPT) and BCG do reduce the risk of TB transmission and the risk of disseminated TB,” Loveday says.
Read in Daily Maverick: “TB treatment can be cut to two months for some, landmark study finds”
According to Schaaf, congenital TB (either catching TB in the mother’s womb or aspirating fluid during the birthing process) is relatively rare and depends on the type of TB that the mother has.
“The greater risk for TB in the baby is when the untreated mother passes on the TB infection to the baby after birth. And because of the baby’s undeveloped immune system, the risk is 50% for the baby to develop TB disease (and often very severe) after infection,” he says.
Risk by numbers
Also presenting at the Union World Conference on Lung Health, Dr Amita Gupta, director of the Division of Infectious Diseases at John Hopkins University’s School of Medicine, said a meta-analysis of 3,384 pregnancies with active TB and 119,448 without active TB consistently found increased adverse outcomes associated with TB in pregnancy.
Mortality was fourfold, morbidity threefold and hospital admissions tenfold. A pregnant woman with TB has nine times more chances of having a miscarriage, two times more of a Caesarean section, and a fourfold risk of developing anaemia, according to the research.
“Having TB during pregnancy is obviously something we want to prevent,” says Gupta.
For perinatal outcomes, there was a fourfold chance of perinatal death, birth asphyxia (failure to start breathing at birth) was fivefold, and low birth weight, preterm birth and acute foetal distress were twofold.
Uncertain burden
“It is estimated that around 200,000 pregnant and postpartum women develop TB each year,” says Schaaf, although he stresses that the actual burden of maternal TB is uncertain.
Mokhele concurs and says the global burden of active TB disease among pregnant women is not well documented. “Available estimates are normally extrapolated using the proportion of TB cases among women in their child-bearing years combined with the crude birth rates. Current available estimates are from 2011 and approximately 216,500 pregnant women were estimated to have TB globally,” she says.
According to Gupta, of the 3.4 million women who fell ill with TB in 2021, we don’t actually know how many of them were pregnant or lactating because those data are not routinely collected.
“But we do believe that the TB burden during pregnancy is high and likely underreported,” she says.
“What we do know also is that the TB incidence peaks during reproductive ages – that is between 25 years to 44 years irrespective of HIV status,” says Gupta.
Effects on infants and adolescents
Loveday says they don’t really know the extent of TB disease or TB mortality in adolescents, since this age group is not reported on to the WHO.
“However, for children aged zero to 14, we know that 1.09 million developed TB in 2020 and 48% of them were [younger] than five years old. We also know that there were 226 000 deaths due to TB in children (0-14) in 2020 and of these deaths 80% were in children [younger] than five – most of whom (96%) did not access treatment,” she says.
Also explaining the risk to infants, Schaaf says infants whose mothers have TB will often develop TB disease and are much more likely to develop severe disease such as miliary TB and TB meningitis.
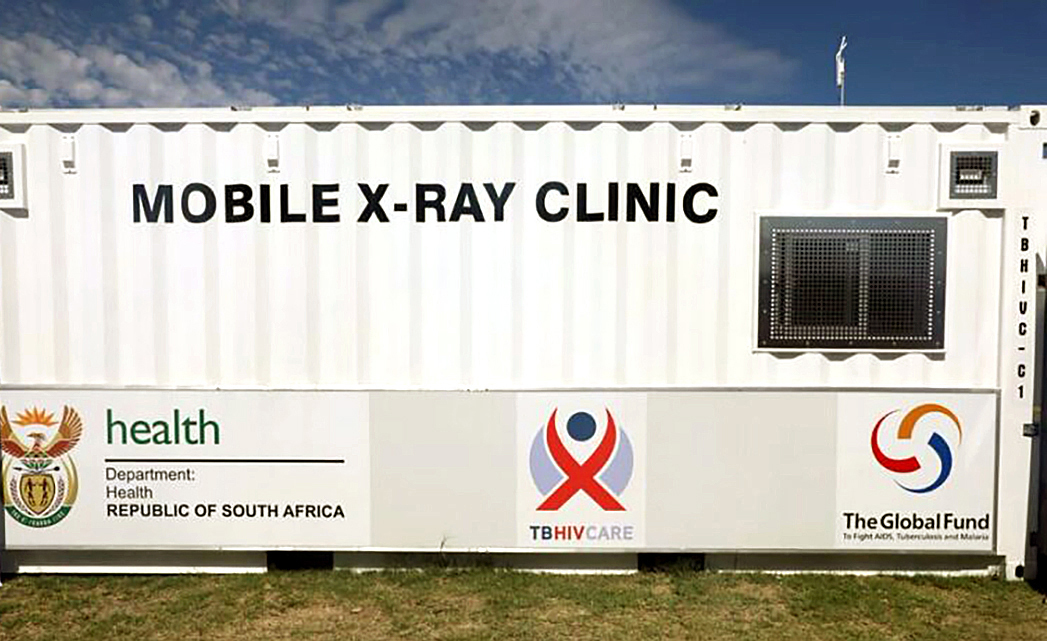
An estimated 200,000 pregnant and postpartum women develop tuberculosis each year, although the actual burden maternal of TB is uncertain. (Photo: WC Health / Spotlight)
“The mortality in these young infants is also often high, as the diagnosis is often delayed because health workers do not always consider TB, especially in young infants. Regarding adolescents, it is rather that they themselves can have TB and become pregnant, or be pregnant and develop TB, especially if they are living with HIV,” he says. Schaaf notes that adolescents need extra care, counselling and support in adhering to TB treatment and other challenges they experience at such a vulnerable age.
As a parent, Beko says she struggled to administer her baby’s medicine. “What was really terrible is that there are no paediatric-friendly formulations for TB. So, when I had to give my child medication, they will tell me to crush a quarter or crush three-quarters and give to the child,” she says. “You know, I felt like I was set up for failure. I felt like I was failing my child because I wasn’t sure from crushing if I was giving her enough medication or [if] I was overdosing her.”
Studies ongoing
Schaaf says there is a move towards providing TB preventive therapy to all household TB contacts of people with infectious TB, “which hopefully will reduce the risk also in pregnancy, but more has to be done regarding community and health worker awareness”.
He says there are ongoing studies among pregnant women to look at dosing and safety of the newer short-course TB preventive therapy regimens.
“For example, 3HP (three months of once-weekly rifapentine plus isoniazid) seems to be effective and safe during pregnancy. The aim is for shorter TB preventive therapy regimens, as the six months of isoniazid only is often not completed,” he says.
Also at the union conference, Dr Francesca Conradie, an infectious diseases researcher in the School of Clinical Medicine at the University of the Witwatersrand, presented briefly on the Beat TB study, which is being conducted in South Africa and is embedded in the national TB programme.
“In this study, we decided that pregnant women could be enrolled and they could be enrolled at any stage of their pregnancy. In order to ensure the safety of participants, an ultrasound [for] foetal anomaly is done before initiation [of] treatment. There are 400 women that have been enrolled in this randomised controlled study, with seven being pregnant and six breastfeeding. Data analysis is still under way in order to understand the pharmacokinetics (PK) in TB drugs,” she says. Pregnant women have often been excluded from important TB studies.
Conradie says there is an increasing body of work demonstrating that PK in pregnant women is not at all different from non-pregnant women in the way they metabolise drugs. “There is more work to be done. Following on the Beat TB study, attention should be paid to the inclusion of pregnant women,” she says. DM/MC
This article was published by Spotlight – health journalism in the public interest.















Comments - Please login in order to comment.